
Intra-abdominal Trauma:
Solid Organs Pt. 1 (Spleen and Liver)
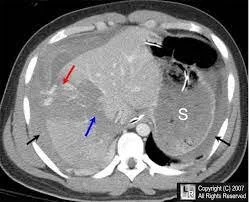
Splenic Trauma
-

Overview
The spleen is the most commonly injured solid abdominal organ.
Injuries to the spleen occur via several mechanisms:
direct compression
tearing of capsule/ parenchyma
Most splenic injuries are self-limited (>90%)
-

Diagnosis
Unstable pt w/ positive FAST- exploratory laparotomy
Stable- CT abdomen w/ IV contrast
***Have a high index of suspicion for splenic injury with rib fractures (especially low fractures)
-
Management
Unstable- exploratory laparotomy
Stable w/ active extravasation- angioembolization
Stable without evidence of bleed- observation/ non-operative management
***splenorraphy
chromic suture
omental patch/topical hemostatic agents
partial resection w/ stapler

Trauma Splenectomy:
midline laparotomy
pack four quadrants/ then remove systematically
retract medially to expose retroperitoneal attachmenets (starting at white line of Toldt
divide peritoneal attachments
gastrosplenic- has SHORT GASTRICS
splenorenal- SPLENIC ARTERY AND VEINS
splenocolic
splenophrenic
clamp and ligate hilar vessels
No drains needed, unless with concern for pancreatic injury
Post Splenectomy Vaccines
S. pneumonia
N. Meningitides
H. influenzae
Liver Trauma
-

Overview
second most injured solid organ in trauma
High mortality rate:
Blunt- 12.5%
Penetrating 22%
Mechanisms:
Compression, shearing, penetrating
-
Diagnosis
Unstable pt w/ positive FAST- exploratory laparotomy
Stable- CT abdomen w/ IV contrast
perihepatic hematoma, hemoperitoneum, parenchymal disruption
-
Management
Unstable w/ positive FAST- exploratory laparotomy
Stable w/ active extravasation- angioembolization
Stable without evidence of bleed- observation/ non-operative management
successful 85-97% of the time
frequent abdominal exams
physiologic stability is important predictor of non-op success
Psuedoaneurysm- angioembolization

from AAST
Algorithm for surgical management of hepatic bleeding
-Suture hepatorrhaphy: 0 chromic on large blunt-tip needle, horizontal mattress
-Pringle maneuver:
- if still bleeding- hepatic vein
-liver laceration can then be explored and any actively bleeding vessels controlled with suture ligation
-Devitalized tissue should be debrided
-drains should be placed when risk for a bile leak
-vascularized pedicle of omentum: reduce bleeding, promote healing

from clinmed international library