Benign Diseases of the Esophagus
Esophageal Anatomy
Has a mucosa, submucosa, and muscularis propria. NO SEROSA
Upper 1/3 is typically striated, while the Lower 2/3 is smooth muscle
Arterial supply
Cervical = inferior thyroid a.
Thoracic = branches off aorta
Abdominal = L gastric a./inferior phrenic a.
Venous drainage = azygous v./hemi-azygous v.
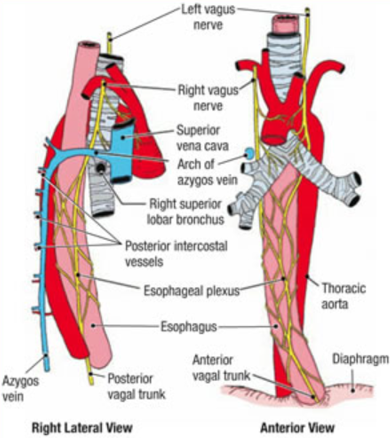
Right vagus n.
Posterior
Cardiac plexus; Criminal nerve of Grassi: persistently high acid levels if undivided after vagotomy
Left vagus n.
Anterior
Liver/biliary tree
Pharyngo-esophageal disorders
Difficulty transferring food from mouth to esophagus
Neuromuscular disease, Myasthenia gravis, Muscular dystrophy, Stroke
Liquids > solids
**Plummer-Vinson syndrome
upper esophageal web + iron deficiency anemia
Tx: dilation, iron, screening for oral cancer
Lower
Epiphrenic Diverticulum
•Associated with motility disorders (achalasia)
•Most commonly in distal 10 cm
•Sx: asymptomatic, dysphagia, regurgitation
•Dx: esophagram, manometry
•Tx: diverticulectomy and esophageal myotomy on opposite side
Upper
Zenker’s Diverticulum
•False diverticulum between pharyngeal constrictors and cricopharyngeus m.
•Failure of cricopharyngeus m. to relax
•Sx: upper esophageal dysphagia, choking, halitosis, regurgitation of undigested food
•Dx: barium swallow, manometry (risk of perforation with EGD)
•Tx: cricopharyngeal myotomy with resection or suspension of diverticulum. IF 3cm or greater, can use transoral stapler
•Left cervical incision +/- drains
Consider Esophagogram on POD #1
Mid
Traction Diverticuli
•True diverticulum
•Most often lateral, in mid-esophagus
•Causes: inflammation, granulomatous disease, tumor
•Sx: dysphagia, regurgitation of undigested food
•Tx:
Asymptomatic: no surgery
Symptomatic: excision and primary closure
Invasive cancer: palliative tx
Achalasia
Cause: lack of peristalsis, failure of LES to relax. Believed to be from an autoimmune/infectious destruction of neuronal ganglion cells
Sx: dysphagia, regurgitation, weight loss, respiratory sx
Manometry findings: ↑LES pressure, Incomplete LES relaxation, No peristalsis (aperistalsis)
DX: Barium swallow: tortuous dilated esophagus, epiphrenic diverticula, “bird’s beak” appearance to distal esophagus, EGD: rule out esophageal cancer (pseudoachalasia)
Tx: balloon dilation of LES (80% effective), Nitrates, CCB
Surgery- Heller myotomy: left thoracotomy, lower esophageal myotomy, partial Nissen fundoplication
Diffuse Esophageal Spasm
Sx: dysphagia, +/- psych history
Manometry: Frequent, strong, non-peristaltic contractions.
NON COORDINATED; Normal LES relaxation
Tx: CCB, trazodone, Heller myotomy (upper and lower)
Surgery less effective
Nutcracker Esophagus
Sx: chest pain +/- dysphagia
Manometry: High-amplitude peristaltic contractions (>180 mmHg)
COORDINATED; Normal LES relaxation
Tx: CCB, trazodone, Heller myotomy (upper and lower)
Surgery less effective
Scleroderma
Esophagus is MC involved organ
Fibrous replacement of smooth muscle
Loss of LES tone; Strictures
Sx: heartburn, dysphagia, massive reflux
Manometry: Low LES pressure; Aperistalsis
Tx: PPI + Reglan, esophagectomy
Schatzki’s Ring
Almost all associated with sliding hiatal hernia
Found at squamocolumnar junction
Sx: dysphagia
Dx: barium swallow
Tx: dilation, PPI (not resection)
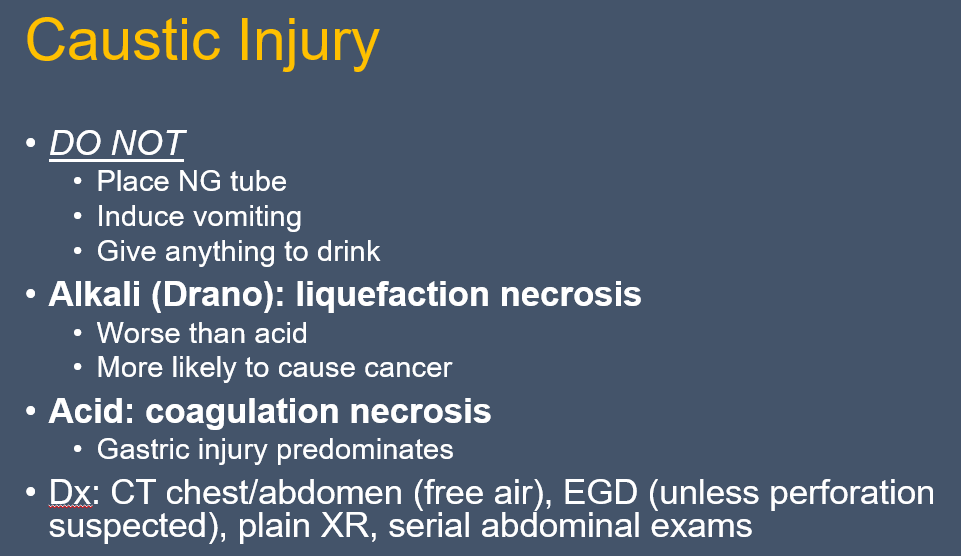
Perforation
MC cause = EGD
MC site = cervical esophagus near cricopharyngeus m.
Natural Narrowings: CP, Aortic Arch, L. Bronchus, GE junction
Sx: pain, dysphagia, tachycardia
Dx: CXR (free air), gastrografin swallow (best test) – No EGD!
Conservative management (NPO, IVF, spit, Abx) if:
Contained perforation
Self-draining
No systemic effects
**Booerhave Syndrome-
•Hx: forceful vomiting followed by chest pain
•Hartmann’s sign: mediastinal crunching on auscultation
•MC left lateral wall 3-5cm above GEJ
•Highest mortality
•Dx: gastrografin swallow